Uterine fibroids: To cut or not to cut?

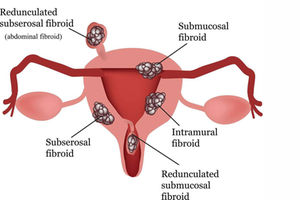
Uterine fibroids (also called leiomyomas) are growths made up of the muscle and connective tissue from the wall of the uterus.

What you need to know:
- Uterine artery embolization is great for women with multiple small fibroids and who have never had surgery on the uterus before. It has a short hospital stay, with low risk of heavy bleeding.
- The patient is monitored for about a day to ensure good pain control after the procedure and is able to get home and resume full function faster.
- However, this is not universally available in our country and it remains financially out of reach for many Kenyans.
Anita* was absolutely done with surgery. She had undergone three surgeries in the past for various non-gynaecological reasons and all the three times, the recovery had been stormy and scary. She did not want to go under the knife ever again.
But here she was, with a fickle little fibroid growing into the cavity of her uterus, causing her absolute chaos. The fibroid was not big but its location was a problem. It led to heavy bleeding every month, with periods lasting seven to eight days, and they were excruciatingly painful.
She had long forgotten about using pads and switched to adult diapers combined with maxi tampons. She was grateful to the pandemic because she now worked from home hence never had to worry about soiling herself while at work.
She lived on iron supplements and all manner of iron-rich foods to replenish the precious red liquid she lost every month. Her social life dwindled to nothing as she didn’t even have the energy to handle anything else beyond work. She spent her free time watching movies and reading about causes of heavy menses in women in their 40s, terrifying herself with the information she came across, from cancer to endometrial hyperplasia, to hormonal imbalance. She had no idea what those were.
She finally collected herself, booked an appointment and came in for a long overdue consultation. After a long chat coupled with an examination, I sent her for tests and her ultrasound found the culprit. She had a few fibroids, nothing remarkable in size, but there was this one fibroid growing into the cavity of the uterus — what is known as a submucous fibroid. That was the genesis of Anita’s woes.
Anita knew enough to know that surgery to remove fibroids or the whole uterus, in general, was the mainstay of treatment. However, the thought of another surgery evoked immediate post-traumatic stress disorder. She was just not ready to get yet another scar. She wanted options that did not involve surgery. At 47, she had a few.
We talked about medical management, where she would receive a special injection that would put her in a state of temporary menopause. This would halt her menstrual cycle and hence do away with the regular monthly bleeding. As long as she wasn’t having menses, she wouldn’t have to experience the heavy blood loss and she would not suffer period pains.
The downside of this was that she would have to deal with the symptoms of menopause much faster and probably in a slightly more exaggerated fashion. She would have to be ready for the hot flashes, anxiety and mood swings, poor sleep, vaginal dryness and possibly even change in appetite.
The injection could be safely administered over a six-month period as either a monthly dose or a three-monthly dose for a period of six months. Thereafter, she could withdraw from it and hope that by the time her cycle re-establishes, she would truly be headed to menopause and hence her symptoms could be alleviated. If the symptoms required continuation of the treatment, she would then require to take hormone replacement therapy to reduce the risk of complications, most notably, osteoporosis.
This is a good option for patients who may agree to surgery but may not be ready for it due to anaemia or other medical conditions that require to be addressed first. The treatment also helps to reduce the size of the fibroids prior to surgery, making the procedure less complicated. It also works well for women with fibroids who are approaching menopause, especially if the fibroids are not big.
I also talked to Anita about uterine artery embolization, a minimally invasive procedure that ameliorates the need for surgery. In this treatment, the patient is sedated and a special probe is inserted into the patient’s large blood vessel in the thigh and goes along the system to the branches of the blood vessels of the uterus itself. The probe is directed to the blood vessels that feed the fibroids and these are sealed off with a special chemical, cutting off blood supply to the actual fibroid. This results in the starvation of the said fibroid with long-term degeneration. It results in reduced period flow, less period pain and potentially can decrease the size of the fibroid.
This is great for women with multiple small fibroids and who have never had surgery on the uterus before. It has a short hospital stay, with low risk of heavy bleeding. The patient is monitored for about a day to ensure good pain control after the procedure and is able to get home and resume full function faster. However, this is not universally available in our country and it remains financially out of reach for many Kenyans. Anita went home and mulled over her options. She promised to discuss it with her family but it was rather obvious where her leanings were. She chose the uterine artery embolization. The procedure was successfully carried out by an interventional radiologist and she had a great response to treatment. She now awaits her menopause in peace and her social life is back in high gear!
Sometimes, we truly do not need to cut!
Dr Bosire is an obstetrician/gynaecologist