Nursing student’s innovation that could transform TB diagnosis

Lewis Lennox, a final-year nursing student at Karatina University (left) and Justin Ongwae, a chest clinic nursing officer, examine a chest radiograph at Karatina Level IV Hospital in Nyeri on May 21, 2025.

What you need to know:
- Traditionally, the analysis of chest X-ray images for TB is done manually by a radiologist or a trained clinician. It involves carefully examining the X-ray for visual signs that may indicate the presence of TB.
At Karatina Sub-county Hospital’s chest clinic in Nyeri County, a quiet revolution is underway. Justine Ongwae, a chest clinic nursing officer, logs into a computer and uploads different chest X-ray images into an Artificial Intelligence (AI) tool before analysing them to detect signs of tuberculosis (TB).
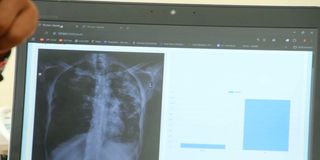
A chest radiograph being investigated for TB using an AI tool at Karatina Level IV Hospital in Nyeri.
With just a click and a few seconds of processing, the AI tool generates results: one patient’s scan shows a 19 per cent probability of TB—indicating a negative result. Mr Ongwae repeats the process for another patient’s image, and the AI returns a 37 per cent probability. Again, no TB detected. However, scans for two other patients show probabilities of 92 per cent and 88 per cent, respectively—both confirming the presence of TB.
This is a third party trial on an AI-powered TB diagnostic software developed by Lewis Lennox, a final-year nursing student at Karatina University. The diagnostic tool is capable of analysing chest x-rays to detect TB and identify the specific strain of infection. With a 92 per cent accuracy rate during early trials, the tool is showing potential of reducing misdiagnosis and improving treatment planning.
Unlike traditional diagnostic methods—which can take days or even weeks to confirm a test—the AI platform delivers results within minutes. “The tool is simple and intuitive,” Lewis explains. “Healthcare workers just log in, upload a patient’s chest x-ray, and download or print the results.”
The process begins with medical personnel signing up or logging into the platform through a secure and personalised account. They then upload a patient's chest X-ray image. AI analyses the image, scanning for markers that indicate the presence of tuberculosis, including strain identification, if applicable. After a few moments, a detailed report is generated, which can be downloaded or printed for use in diagnosis and treatment planning.
Traditionally, the analysis of chest X-ray images for TB is done manually by a radiologist or a trained clinician. It involves carefully examining the X-ray for visual signs that may indicate the presence of TB.
“The common indicators we look for include lung infiltrates or opacities—especially in the upper lobes—cavitations (which appear as holes in the lung tissue), pleural effusions (fluid around the lungs), and signs of fibrosis or enlarged lymph nodes,” explains Mr Ongwae.
However, he adds, an X-ray alone is not enough to make a definitive diagnosis. “The findings are typically interpreted in the context of a patient's symptoms and medical history. For example, if a patient presents with a persistent cough, unexplained weight loss, night sweats, or a known exposure to TB or HIV, these clinical details are considered alongside the imaging results to guide further testing or diagnosis.”
Mr Ongwae explains that traditional diagnosis may require more scrutiny and additional testing to ensure accuracy, particularly in cases where the X-ray findings are subtle or ambiguous.
A radiologist can review and interpret a chest X-ray within minutes. But if TB is suspected, additional diagnostic tests are often necessary to confirm it. “These may include sputum microscopy, which can provide same-day results, the GeneXpert MTB/RIF test, which gives results in a few hours, or a culture test—considered the gold standard—which can take up to six to eight weeks,” adds Mr Ongwae.
Affordability, Lewis says, is at the heart of the AI platform’s mission, with a pricing model carefully designed to accommodate a wide range of users and healthcare settings. For those who prefer not to commit to a subscription, the platform offers a pay-per-use option, charging between Sh100 and Sh250 for each image analysis. “This allows flexibility for clinics and practitioners who may only need occasional access," he says.
For frequent users, he plans to charge Sh50,000 and Sh60,000 every six months, while annual subscribers will be parting with Sh90,000 to Sh100,000 per year.
“This tiered pricing structure ensures that the platform remains accessible not only to large hospitals and institutions, but also to small rural clinics and healthcare providers operating under tight budget constraints,” explains Lewis.
By offering multiple payment options, he says, the platform aims to eliminate cost as a barrier to quality TB screening and diagnosis. “By providing a low-cost, high-accuracy diagnostic alternative, we aim to empower frontline healthcare workers to diagnose TB accurately and rapidly, even in remote areas."
Target partners
Key target partners include the Ministry of Health in Kenya, county governments, and both public and private hospitals. The tool is also positioned for adoption by diagnostic and imaging centers, medical training institutions, and research organisations.
But even with these promising results, the road is still long before this prototype is brought to full-scale implementation. According to Lewis, a few critical steps remain before the tool becomes fully functional and approved for broader use.
“We are currently preparing to submit comprehensive documentation to several regulatory bodies, including the Kenya Medical Practitioners and Dentists Council, the Radiologist Board, the Pharmacy and Poisons Board (PPB), and the Kenya Medical Devices Authority.”
This submission, Lewis says, will include trial data, clinical validation reports, and risk assessments to support official evaluation and approval of the product. Building on the success of initial trials, he also plans to conduct multi-site clinical validation to ensure consistent accuracy and performance across diverse populations and healthcare settings.
Additionally, Lewis explains that he is working to integrate the software with Kenya’s TIBU system and various hospital Electronic Medical Records to facilitate seamless reporting, case management, and patient follow-up.”
Lewis says he is seeking funding and partnerships to bring his prototype to full implementation. “Together, we can create a future where no one in Kenya—or Africa—dies because of late or incorrect TB diagnosis.”
If successful, this could be a game-changer for TB detection in Kenya and beyond.




