Born into pain: The hidden burden of sickle cell in Kenya

Betty Anyango Odero, founder of Nia Health Community Based Organisation, which empowers children, adolescents, and young people with sickle cell disease in informal settlements. She is also a sickle cell carrier and mother to sickle cell warriors.
What you need to know:
- According to the Ministry of Health, an estimated 14,000 children are born with sickle cell disease annually in Kenya, making it a significant contributor to child and adult mortality and health complications.
Whenever one of her children was admitted to hospital, Betty Anyango remained behind as other parents walked out with theirs. She could be in the wards for days. Sometimes the stay stretched into weeks. This happened so many times that the nurses and doctors at her local hospital know her by name.
Betty is a mother of five. Four of her children were born with sickle cell disease. One is a carrier. She has lost two of them.
"I am a mother of five children: four with sickle cell, and one who is a carrier. Out of the four, I lost two," she says, fighting back tears.
For nearly three decades, sickle cell disease has shaped her life in ways she never imagined, the sleepless nights, the mounting hospital bills, the days missed from work, and the quiet grief of burying a child. Across Kenya, thousands of families start this same journey every year
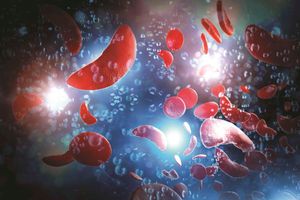
Sickle cell disease (SCD) is a group of inherited blood disorders that affect haemoglobin, the major protein in red blood cells responsible for carrying oxygen through the body. In healthy individuals, red blood cells are disc-shaped and flexible, allowing them to move easily through blood vessels. In people with SCD, a gene mutation causes the cells to take on a crescent or sickle shape, preventing oxygen from flowing freely to the rest of the body and triggering what are known as painful crises.
Globally, Africa bears the largest burden of the disease. Of the approximately 400,000 babies born with sickle cell disease every year, more than 67 per cent are born on the continent. In many African countries, between 50 and 90 per cent of affected children die before the age of five, largely due to the absence of early screening and access to appropriate care.
In Kenya, the Ministry of Health estimates that 14,000 children are born with sickle cell disease every year. The condition is most prevalent in malaria-endemic areas, Nyanza, Western and coastal regions, though it is becoming a growing national concern.
"We have had people from the three burdened regions getting married across the country, and the result is an increase in the number of carriers and SCD warriors," says Dr Phionah Obanda, a genomic scientist based in Vihiga County.
Dr Obanda says the response must go beyond the most affected counties. "We need to have a database of all people and their sickle cell status so that we can help them make informed choices," she adds.
For Betty, the disease did not announce itself immediately. Her first child appeared healthy and energetic through infancy, but shortly after his first birthday, he began crying constantly. Any touch caused him pain.
"He started crying constantly. He felt pain when touched anywhere. I could not understand what was happening," she recalls. She took him to a paediatrician and tests confirmed he had SCD. It was only then that the mother of five learnt she was herself a carrier.
Her second child also appeared healthy at birth but died at just 10 months after developing subacute malaria. A peripheral blood film, a diagnostic test that examines a blood sample under a microscope to identify sickle-shaped red blood cells, was positive.
By the time her third child was born, Betty sought early testing. The results confirmed the blood disorder. Her fourth child was also diagnosed with sickle cell disease, and the fifth tested negative but was later found to be a carrier.
"It was very difficult. I lived in western Kenya where malaria is common, so the children were often sick. I was constantly in and out of hospital. Balancing work and caregiving became an enormous challenge. You go to work, but about two days in the week you are out because one child is sick. You basically live in the hospital," she says.
The emotional burden was overwhelming.
"When a child has a high fever or is in pain, you cannot sleep. It breaks your heart because you know they are suffering and they cannot live like other children. Sickle cell crises are often accompanied by severe pain. As a mother, you feel that pain with them," she says.
The financial strain was equally heavy. Children with sickle cell require stronger antibiotics and longer hospital stays than other children. Betty would watch other parents leave the ward while she remained, her bills climbing by the day.
"By the time you clear the bill, it has skyrocketed. I was working, so I managed somehow, but I saw mothers who were casual labourers or peasant farmers. Their situation was devastating," she says.
Betty grew up in Migori County, second-born in a polygamous family of nine siblings. Only five of the nine survived childhood. The other four died from childhood illnesses, but Betty never knew the cause. Sickle cell disease was never raised as a possibility.
The greatest loss came when her firstborn died at the age of 20, in his second year at university.
"He died due to sickle cell disease. The loss plunged me into deep grief. After some time, I told myself I had to rise again," she says.
Before his death, her son had repeatedly spoken about doing more for others living with the condition. He would ask his mother to buy medicine for friends who had the disease. He invited them home to cook and eat together. At one point, he asked her to develop a concept for supporting children living with chronic illnesses, including sickle cell disease, epilepsy and autism, among them.
"After he died, I decided I would honour him by doing what he had wanted," says Betty.
She went on to establish Nia Health Assist, a community-based organisation in Kibera that supports children living with sickle cell disease and their caregivers. The
organisation currently supports 32 needy children and their families, most of them from informal settlements in Nairobi. Some of the children were abandoned by their parents in dire circumstances.
"We bring caregivers together so they can share their experiences and learn from each other. Many families arrive burdened not only by the disease but also by stigma and misinformation," she says.
Through counselling sessions and community discussions, Betty helps caregivers understand the medical reality of the disease and how to manage it. Nutrition is also a central focus.
"These children need balanced meals with high protein and vitamins. Fresh vegetables and fruits help strengthen their immune systems. However, many families struggle to meet even the most basic nutritional needs," she says.
The organisation runs a small feeding programme where caregivers prepare and share meals. "We cook simple food — beans, rice and vegetables, sometimes chapati and fruits. It becomes a good time where the children and caregivers can eat and talk," says Betty.
Resources remain stretched, more so at home, where Betty also cares for her mother, who is battling cancer.
"The biggest challenge we face is funding. Many families also struggle to afford health insurance and routine clinic visits. Some cannot afford the annual contribution for health coverage. Even clinic visits require money for tests and medication," she says.
The challenges Betty describes on the ground are well-documented at the clinical and policy level.
Prof Constance Tenge, a paediatrician at Moi University and a member of the scientific committee of the Sickle Cell Federation of Kenya, says that despite progress in managing the condition, significant gaps remain, driven largely by unreliable data on the number of warriors.
While the Ministry of Health puts the figure at 14,000 children born with SCD annually, Prof Tenge says many more cases go undocumented because of the absence of screening and testing services; this, even though the number of health professionals attending to people with the condition has grown considerably over the years.
In 2022, the professor and fellow researchers set out to assess the level of knowledge among healthcare providers about SCD, evaluate existing healthcare services for warriors, and register those living with the condition across Bungoma, Busia, Kakamega, Vihiga and Trans Nzoia counties.
The study assessed 76 health facilities. While the facilities had laboratory and pharmacy departments and both skilled and unskilled healthcare providers, services for SCD warriors were largely unavailable due to shortages of medicines, equipment and supplies.
Prof Tenge shared the findings during a recent SCD conference held in Kisumu at Jaramogi Oginga Odinga Teaching and Referral Hospital.
Of the 2,056 people living with SCD who were interviewed during the study, only 34.1 per cent had active and useful medical cover. The remaining 66 per cent were locked out entirely.
Only 30.8 per cent of the warriors were able to access and afford hydroxyurea, the key drug used in managing the condition. And only 17.3 per cent had undergone a confirmatory test to diagnose sickle cell disease, largely because of a lack of equipment. The test is critical in identifying, quantifying and separating different haemoglobin types among those living with the blood disorder.
One of the major challenges identified by the study was the absence of reliable data, which continues to widen the medical supplies gap in the burdened counties.
In Kakamega, one of the counties most affected by SCD, warriors and advocates have responded by establishing a revolving fund pharmacy to ensure a reliable supply of medication to patients when they need it. The initiative has so far registered more than 450 clients.
"We are yet to get updated data on the state of the blood disorder in the county," says Hillary Kosano, an SCD advocate from Kakamega, adding that the county is working towards setting up SCD screening services within reach of its residents.
The situation is not very different in neighbouring Bungoma and Vihiga counties, where many people still believe the condition is a curse and rarely visit health facilities for expert management.
To address the data gap, the researchers designed a standardised form to collect information on people living with SCD, covering demographics, family details, clinic locations, services received, medication administered, and whether patients are able to use them. The aim is to build a registry that can be shared with counties, donors and the Ministry of Health for planning, policy development and budget allocation.
"When put into practice, the data in the forms can be shared with counties, sponsors and the Ministry of Health for planning, coming up with policies and enough budgetary allocations," says Prof Tenge.
She adds that the recommendation for a national registry was handed to the Ministry of Health in October 2025 for consideration.
The researcher is also calling for expanded screening services across the country, for both children and adults. While many adults prefer to be tested when preparing to settle into relationships, she says the right time is during adolescence.
"Adolescents are in a position to understand information on the disease. At that stage, they are also not yet in stable relationships. I would advise that you screen the child at the infancy stage and then catch up with them during adolescence for a full understanding of what their status means," she says.
On the regional front, Kenya and Tanzania have joined hands with civil society in an initiative called the SCD-KeTan project, aimed at reducing deaths and complications caused by sickle cell disease in East Africa.
In Kenya, partners in the initiative include the Ministry of Health, the Sickle Cell Federation, the Children Sickle Cell Foundation, the Africa Sickle Cell Organisation and the Sickle Cell Awareness Foundation. In Tanzania, partners include the Ministry of Health, the Tanzanian Sickle Cell Alliance, the Bone and Blood Foundation, TASIWA and the Zanzibar Faculty of Health Sciences.
The project, running from May 1, 2025 to April 30, 2028, aims to improve early diagnosis, expand access to medical care, and build the capacity of health systems and civil society organisations working in the sickle cell space.
Its total budget is €3.1 million (approximately Sh430 million), funded by the Agence Française de Développement, which is contributing 76 per cent, and the Fondation Pierre Fabre, which is providing the remaining 24 per cent.
By the close of the project, the initiative aims to screen 70,000 new-borns and infants, test 20,000 children during paediatric consultations, and offer voluntary screening to 38,000 people. Screening will be conducted during routine paediatric consultations and through voluntary testing programmes in schools and communities.
Beyond testing, the project will work to improve access to care by supporting enrolment of patients in health insurance schemes, strengthening medical follow-up, and establishing revolving pharmacy funds for essential medicines. It will also train 1,400 health professionals, support 1,600 children living with sickle cell disease, and provide psychosocial and economic support to 1,700 patients and families.
Six civil society organisations will be strengthened under the initiative, and support will be extended to two federations of patient associations in the sickle cell space.
Economic support activities, including income-generating projects to help families manage the financial burden of the disease, will also be part of the programme, alongside public awareness campaigns in communities and schools aimed at reducing stigma and improving understanding of the genetic condition.